⚕️ Medical Disclaimer
This content is for informational purposes only and does not constitute medical advice. Always consult your GP or prescribing clinician before making changes to your medication, diet, or supplement regimen.
⚡ QUICK ANSWER
What is a healthy BMI in the UK?
In the UK, the NHS defines a healthy BMI as 18.5 to 24.9 kg/m². BMI of 25-29.9 is classified as overweight; 30-34.9 as obese class I; 35-39.9 as obese class II; 40+ as obese class III. For South Asian, Chinese, Black African, and African-Caribbean populations, health risk thresholds are lower — 23+ is considered overweight and 27.5+ obese for these groups.
BMI is the most commonly used screening tool for weight-related health risk in the UK — it determines NHS treatment eligibility, is used in NICE guidelines, and forms the basis of most clinical weight management decisions. Understanding what it measures, where it is reliable, and where it falls short helps you interpret your own health picture more accurately. For GLP-1 eligibility specifically: Am I Eligible for Mounjaro UK?.
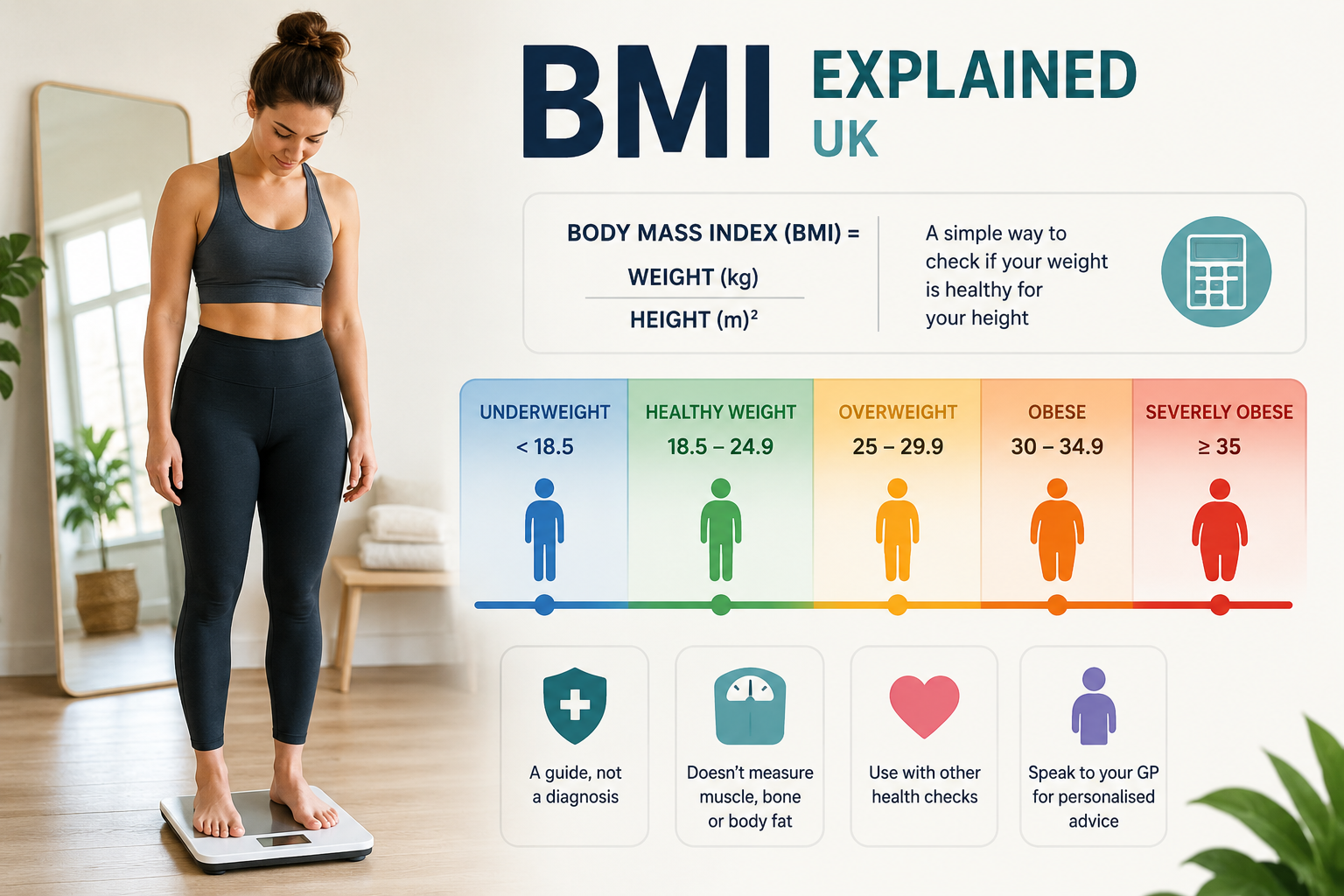
What BMI Actually Measures
BMI (Body Mass Index) is calculated as: weight (kg) ÷ height (m)². It is a simple ratio of weight to height — nothing more. It does not directly measure body fat, muscle mass, fat distribution, metabolic health, or any other biological marker. It is a screening statistic that correlates with health risk at a population level — meaning it works reasonably well across large groups but is less reliable for individuals.
| BMI Category | BMI Range (UK NHS) | Adjusted Range (South Asian, Chinese, Black African/Caribbean) |
|---|---|---|
| Underweight | Under 18.5 | Under 18.5 (same) |
| Healthy weight | 18.5 to 24.9 | 18.5 to 22.9 |
| Overweight | 25 to 29.9 | 23 to 27.4 |
| Obese (Class I) | 30 to 34.9 | 27.5 to 32.4 |
| Obese (Class II) | 35 to 39.9 | 32.5 to 37.4 |
| Obese (Class III) | 40 and above | 37.5 and above |
Why BMI Is Useful
- Population-level risk correlation: At a statistical level, higher BMI is consistently associated with increased risk of type 2 diabetes, cardiovascular disease, certain cancers, and joint disease
- Consistency: It is calculated the same way by every healthcare professional — making it a reliable communication tool
- Speed and simplicity: Calculable in 10 seconds from two measurements already taken at most GP appointments
- Treatment eligibility: NHS and NICE guidelines use BMI thresholds because they provide a consistent, defensible eligibility criterion
The Significant Limitations of BMI
BMI’s limitations are well-established in the clinical literature — it remains in use because of its simplicity, not because it is the most accurate tool:
| Limitation | Why It Matters | Example |
|---|---|---|
| Does not distinguish fat from muscle | High BMI in very muscular people classifies them as overweight or obese | A rugby player with 10% body fat may have a BMI of 28-30 |
| Does not measure fat distribution | Visceral (abdominal) fat is more metabolically dangerous than subcutaneous fat; two people with the same BMI can have very different risk profiles | A person with a BMI of 27 with most fat centrally is at much higher risk than the same BMI with fat distributed peripherally |
| Does not capture metabolic health | Some people at BMI 30 are metabolically healthy; others at BMI 25 are not | The ‘metabolically healthy obese’ and ‘normal weight obese’ concepts are well-documented in research |
| Ethnic variation is significant | The adjusted thresholds for South Asian and Black populations reflect this — but many clinical systems still use generic ranges | South Asian populations develop type 2 diabetes at significantly lower BMI than white European populations |
| Sex differences in fat distribution | Women naturally carry more fat than men at the same BMI; this is healthy and normal — but BMI does not reflect this difference | A woman and a man with the same BMI have meaningfully different body compositions |
💡 Waist-to-Height Ratio Is Often More Useful Than BMI
A waist-to-height ratio under 0.5 (your waist circumference should be less than half your height) is a better predictor of metabolic risk than BMI alone. Measure your waist at its narrowest point. Divide by your height (both in the same unit). Under 0.5 = low risk; 0.5-0.6 = increased risk; over 0.6 = high risk.
Better Measures to Use Alongside BMI
| Measure | How to Take It | Healthy Range | What It Tells You |
|---|---|---|---|
| Waist circumference | Around natural waist, at end of normal exhale | Under 80cm (women), under 94cm (men) | Central obesity — the most metabolically dangerous fat pattern |
| Waist-to-height ratio | Waist cm ÷ height cm | Under 0.5 | Visceral fat risk — better cardiovascular predictor than BMI |
| HbA1c (blood test) | Via GP blood test | Under 42 mmol/mol (non-diabetic range) | 3-month average blood sugar — direct metabolic health marker |
| Blood pressure | At GP or pharmacy | Under 120/80 mmHg (optimal); under 130/85 acceptable | Cardiovascular risk — directly affected by weight |
| Resting heart rate | Morning, before getting up | 50-70 bpm (fit); under 100 bpm (normal) | Cardiovascular fitness — improves with weight loss and exercise |
BMI and GLP-1 Eligibility in the UK
NHS NICE guidelines use BMI as the primary eligibility criterion for GLP-1 weight management treatment because it provides a consistent, documentable threshold. The specific thresholds (35+ for most; 32.5+ for some ethnic groups) are not arbitrary — they represent the points at which the evidence for treatment benefit clearly outweighs risk. Full eligibility guide: Am I Eligible for Mounjaro UK?.
Private clinics use lower BMI thresholds (27+ with comorbidities; 30+ without) because they operate outside NICE cost-effectiveness constraints and can offer treatment to people where the benefit-risk profile is still positive, even if NHS resources are not allocated to that level.
RECOMMENDED SUPPLEMENTS
Lily & Loaf — Quality Supplements for GLP-1 Users
Whatever your starting BMI — these supplements support the metabolic and nutritional foundations of sustainable weight loss.
📚 RELATED READING
Some links in this post are affiliate links. If you purchase through them, I may earn a small commission at no extra cost to you. I only recommend products I use myself. Use code ALAN10 for 10% off Lily & Loaf. This post is for informational purposes only — always consult your GP for medical advice.
The Future of BMI in UK Medicine
NICE and NHS England have been reviewing whether BMI should remain the primary screening criterion for weight management treatment. The emerging consensus is that BMI should be supplemented with waist circumference and a measure of metabolic health (HbA1c, blood pressure, lipid panel) rather than replaced entirely. Several proposals for ‘metabolic BMI’ or composite scoring are in clinical discussion as of 2026.
For now: BMI remains the practical gating criterion for NHS and private GLP-1 eligibility. Understanding its limitations helps you make the case for treatment if your BMI is borderline but your metabolic health markers tell a different story.
Sources: NICE: obesity overview and guidance review 2024 · NHS England: review of weight management treatment eligibility · Caleyachetty et al., 2021: BMI misclassification and cardiometabolic risk
Discover more from Healthy Weight Loss GLP1
Subscribe to get the latest posts sent to your email.